Women, obesity, and what we didn’t see
MISSED. MISREAD. MINUSED.
A Women’s Day Special 2026
It all starts well.
In India, millions of women are being told to lose weight.
Few are ever told how they gained it. Obesity in Indian women often develops gradually — influenced by underlying biology, shifting life stages, and broader systems that have not fully accounted for women’s health needs.
This is not a report about willpower or failure. It is instead a story about what was missed, what might have been misread, and what we may have unintentionally left out along the way.
This is Ananya’s story.
And it is far more common than we think.
The body that looked fine
Ananya was healthy.
In her early twenties, her weight stayed within what doctors called “normal.”
Her BMI didn’t cross any alarming threshold. No one told her that exercise was a habit she had to get into now. No one told her that hanging out with friends wasn’t all about pizzas and parties.
From the outside, her body looked fine. And in medicine, what looks fine often is fine — until it isn’t.
What BMI couldn’t see was where fat was settling: around the abdomen, deep inside, quietly shaping her metabolic future. Ananya didn’t miss the warning signs. They were simply never shown to her.
When risk was invisible
Ananya is not an exception. She belongs to a large, overlooked group of women whose bodies carry metabolic risk without carrying visible weight. They move through clinics and check-ups without raising alarms because their numbers fall within range — even when their risk does not.
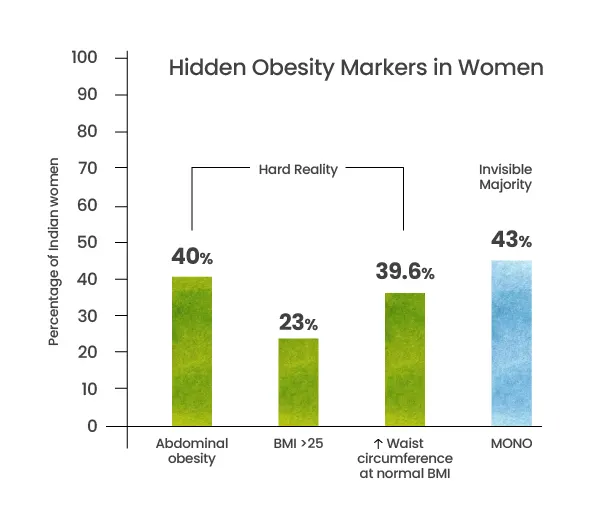
Hard Reality :
- • 40% of Indian women have abdominal obesity (waist circumference > 80 cm).
- • Only 23% of women cross a BMI of 25 (overweight/obese classification).
- • 39.6% exceed the waist circumference cut-off despite a “normal” BMI.
In other words, BMI often fails to flag the biggest risk group — women
whose weight looks acceptable while their waistline tells a different story.
The Invisible Majority
- • 43% of Indians fall under MONO — Metabolically Obese, Normal BMI.
- • 1.7X more women are metabolically dysfunctional than visibly obese.
This is what was missed early: risk that didn’t fit the checklist. And what is
missed early is often misread later.
When age adds more than just years
In her late twenties, Ananya felt fine. Small changes were easy to dismiss. Fatigue had explanations. Weight shifts were temporary. No one spoke about how metabolic risk accumulates with age — even without dramatic weight gain. By the time women like Ananya reach their thirties, the body has already begun to change.
Not suddenly. Not visibly.
But decisively.
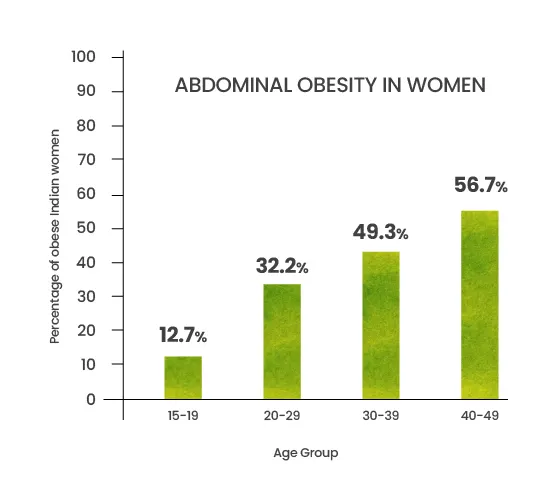
Hard Reality (India): Abdominal Obesity by Age (Women)
- • 15–19 years: 12.7%
- • 20–29 years: 32.2%
- • 30–39 years: 49.3%
- • 40–49 years: 56.7%
By the late thirties, nearly one in two women already carry abdominal obesity — often without knowing it.
When life was mistaken for choice
In her mid thirties, life sped up. Work became heavier. Responsibilities multiplied. Time became something to manage, not own. Sleep became a luxury. Empty calories mounted along with everyday pressures.
Ananya’s weight shifted again — not dramatically, but steadily. Everyone had an explanation: stress, marriage, age, “this happens.”
Ananya believed them. So did the system.
The Postpartum Reality
- • Mean weight retention: 5.0–5.8 kg at 3–6+ months1
- • Excess gestational weight gain higher long-term retention
- • C-section deliveries: 27.9% retain ≥10 pounds at 12 months2
- • Breastfeeding adds 500+ kcal/day demand without structural nutritional support3
Cultural & System Drivers
- • “40-day confinement” ghee-heavy, high-calorie diets4
- • Sleep deprivation cortisol & appetite dysregulation. women with less than 5 hours of sleep are 2–3 times more likely to retain more than 5 kg postpartum5
Signals That Didn’t Seem Urgent
It was soon time for another child. Around this time, Ananya was told she might have PCOS. Not urgently. Not definitively. It was framed more as a reproductive issue — not a metabolic one. She was advised to eat better, move more, manage stress. PCOS became a background label: acknowledged, but not explored.
PCOS was not the problem. It was a signal.
The Missed Reality
- • PCOS is the most common endocrine disorder in reproductive-aged women
- • It is a primary driver of early-onset obesity in Indian women
- • ~20% of reproductive age Indian women are affected
Life Transitions Without Reset
As the years passed, weight gained during stressful periods didn’t fully come off. Sleep became lighter. Energy dipped more often.
Each change had a reasonable explanation. None felt urgent enough to interrupt life. What was happening wasn’t failure.
It was cumulative adaptation. Eventually, the advice became clearer: “Lose weight.”
“Improve your lifestyle.”
The journey that brought her here disappeared.
This is what misreading looks like: we mistake adaptation for indiscipline.
We treat cumulative biology as personal choice.
MINUSED
The Slow Subtraction
Nothing in Ananya’s life was taken away all at once. That’s why it was
hard to notice.
Meals were regular. Calories were sufficient. But nutrition thinned. Protein
was optional. Vegetables were inconsistent. Carbohydrates were
dependable.
She often ate last.
She often ate less.
Not by choice — by rhythm.
Women frequently experience protein and micro nutrient deficiencies even when calorie intake is adequate. Obesity and under nutrition can coexist — and standard weight-loss advice often misses this paradox.1
Cultural Context : The Nutritional Paradox : Caloric Excess, Micro nutrient Deficiency
- • Women eat last and smallest portions in joint family settings2 Processed foods are affordable, accessible status symbols but nutritionally inadequate3
- • Breastfeeding mothers receive cultural validation to “eat more” but not nutritional guidance4
- • Postpartum “tonics” are high-calorie, high-sugar, marketed as health but metabolically risky4
Sleep, Deferred Care, And What Disappears
Sleep wasn’t sacrificed – it was interrupted: late nights, early mornings, mental lists that never switched off.
Sleep deprivation amplifies: Abdominal fat storage, Cravings for refined carbohydrates Hormonal imbalance across life stages2
Preventive care followed the same pattern. Appointments were postponed. Nothing felt urgent enough to priorities.
Women often seek care later than men for non-acute conditions, delaying metabolic diagnosis.
What she gained in weight, she lost in resilience.
In A Few Years Time
In a few years, Ananya’s body will change again.
As she moves into her fifties and early menopause, fat will
settle more firmly around the abdomen. Muscle mass will
decline quietly. Insulin sensitivity will shift again.
This time, the changes will be harder to ignore.
The Timeline Revealed
What was missed early compounded.
What was misread went uncorrected.
What was minused surfaced.
Obesity is not a phase.
It is not a single failure.
It is a timeline.
- • 56.7% of women aged 40–49 have abdominal obesity, even when overall weight gain appears modest.
What shows up now is not new. It is the visible sum of everything that came before.
Editor’s Note
This story is not meant to offer answers, but to reframe the question.
Women’s obesity in India cannot be understood through a single lens — not diet alone, not hormones alone, not lifestyle alone. It sits at the intersection of biology, life stages, food systems, care giving roles, and healthcare models that were never designed to see women fully.
At Brandcare, we believe meaningful progress in women’s health begins by listening deeper, and resisting one-size-fits-all narratives.
Because before solutions can work, the story itself has to be told right.
About BrandCare
BrandCare is where science meets storytelling—and where healthcare marketing learns to speak human again.
For over two decades, we have helped health and wellness brands find meaning in a world crowded with messages. We translate medical science into ideas that move people—ideas that are grounded in truth, empathy, and a touch of wit.
We are not trend chasers, we are sense makers. We watch how culture, care, and consumer behaviour shift, and help brands stay relevant by staying real. Whether it is guiding a digital transformation, decoding the new physician mindset, or crafting a festive wellness reset, we bring thought leadership that listens before it speaks.
One Reply to “Women, obesity, and what we didn’t see”
hi